

Newsletter
September
2016
The last assessment wave has now already been completed for over a year. However, analysing the collected data will keep us busy for years to come. For this reason, we would like to continue informing you about the results. This newsletter deals with two very reallife topics: quality of life in relation to health status, and what we see as a very important issue - bullying. We hope the summaries are sufficiently understandable. If you would like to read the original papers (unfortunately all in English, but that is the language of science), they can soon be found on the website. Here are the new findings:
1. Preterm birth, bullying, and emotional problems in school age
All children and adolescents sometimes have different opinions than their peers or have conflicts with others. Through this, they learn to negotiate and find solutions with one another.
Bullying is something different. In bullying, a person or a group attempts to systematically inflict harm on a peer and then does so repeatedly, often several times a week, over months or years. It is difficult to defend oneself against it. Bullying can be direct, e.g. through hitting, blackmail or insults, or indirect, through the spreading of rumours or systematic exclusion from activities (play, meetings, leisure activities). Nowadays this can often also be supported by electronic media, from text messages to posts on social media (e.g. Facebook, blogs, Twitter, etc.).
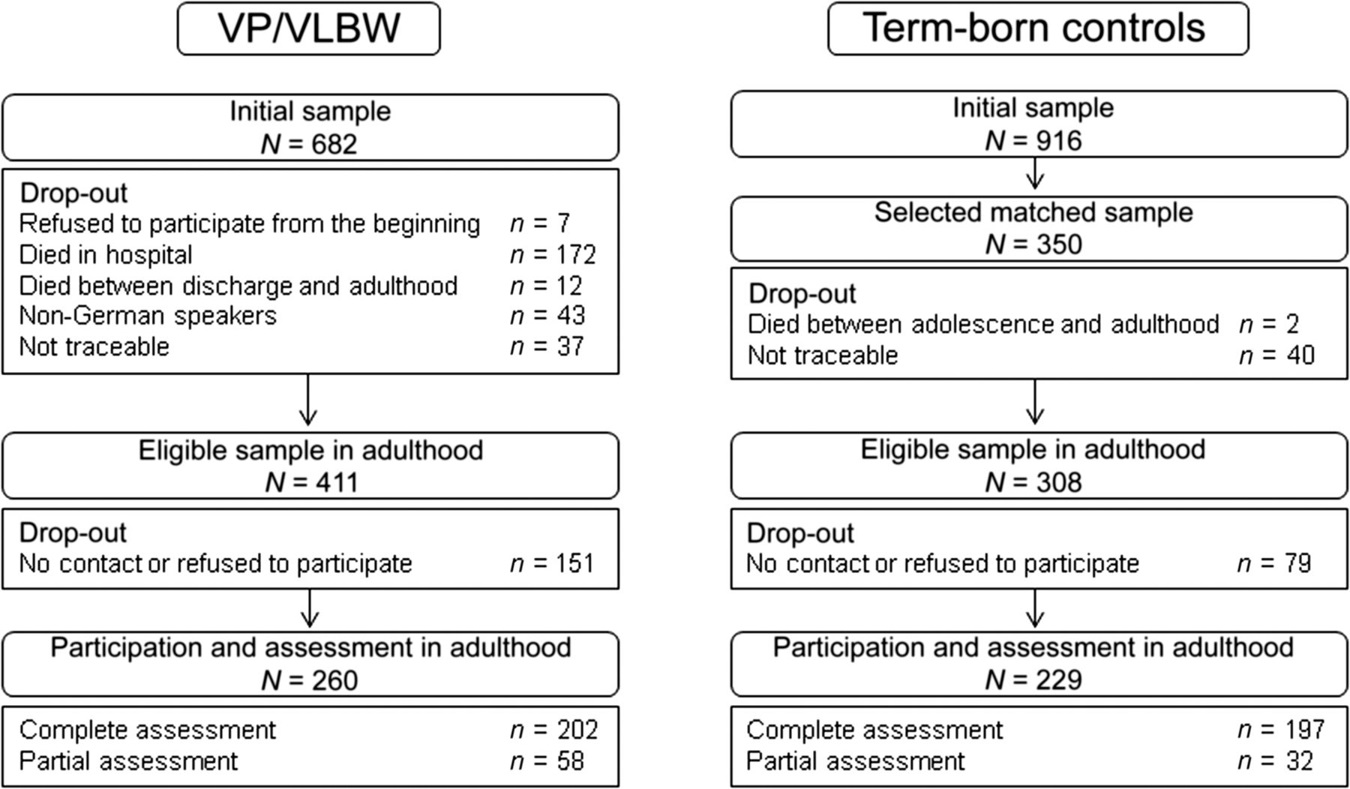
About our study: We asked parents about bullying of their children. These children lived in Bavaria (Bavarian Longitudinal Study) or in Great Britain (EPICure Study) and were in the 2nd and 6th/7th year of school. In both studies we also asked the parents, when the children were in the 6th/7th year of school, to assess their children’s emotional problems (e.g. anxiety, worries, sadness). Both studies examined very or extremely pretermborn children as well as fullterm children.
As already shown in other studies, we found that bullying is not uncommon and that about onequarter to onethird of children have experienced bullying at school, both in Germany and in Great Britain. In both countries, bullying increased with age.
New in our findings is that pretermborn children in both countries, especially as adolescents, had twice the risk of becoming victims of bullying compared to fullterm children. We also found—regardless of whether preterm or fullterm—that those who were chronically bullied over years developed emotional problems more frequently in the 6th/7th school year.
Why are very preterm children bullied more often? This is less related to the fact that they are often somewhat smaller and slighter in build, and more due to the fact that they are more often shy and withdrawn in their personality. Bullies look for children who are easy targets, who do not defend themselves and show quick reactions (e.g. running away, crying), and who have few peers who stand by them.
It is important that parents are always open to their children and that children can talk to them in confidence about bullying.
2. Healthrelated quality of life of very pretermborn individuals
It is known that limitations in health can impair quality of life. In contrast to objective health assessments (e.g., in the context of a medical diagnosis), healthrelated quality of life concerns the respondent’s perception and experience of health impairments and includes physical wellbeing, emotional condition, and social situation.
While most very preterm infants develop healthily, they do nevertheless more often have health impairments that can affect quality of life into adulthood. Therefore, we examined how the quality of life of very pretermborn individuals changes from adolescence to adulthood in the Bavarian Longitudinal Study. We conducted surveys with our study participants themselves, but their parents also provided assessments. The questions on quality of life referred to vision and hearing, linguistic, motor, cognitive, and emotional development and functioning, as well as the occurrence of pain (example of a response regarding vision: “Can see printed text or a friend on the other side of the street well enough, but with glasses”).
Our results show that, on average, pretermborn individuals themselves do not report lower quality of life in adolescence than fullterm individuals, although parents already rate quality of life as lower during adolescence. Interestingly, both fullterm and pretermborn individuals rate their quality of life as suboptimal in adolescence. This may be due to adolescents going through a turbulent stage of puberty and generally judging their lives more negatively. While the quality of life of fulltermborn individuals improved from adolescence to adulthood — both in selfratings and in parent ratings — this was not the case for the pretermborn group or for their parents’ assessments. For pretermborn individuals, perceived quality of life remained at the same level into adulthood, from both their own perspective and that of their parents. Parents reported the lowest quality of life for those adolescents and adults who suffer from severe disabilities (see graphic).
We found that adult study participants and their parents, regardless of whether they were born preterm or at term, rated their quality of life as better when the young adults had friends and a stable relationship, through which they received good emotional support, and were not dependent on social welfare. For quality of life, it is therefore important to be socially integrated and emotionally supported, and to have paid employment.
Subjective assessments and perceptions of health and healthrelated quality of life provide valuable complementary information to objective health findings and can help plan and tailor treatments, interventions, and other healthrelated measures. Our findings show how important it is always to examine the viewpoint and assessment of the affected individuals themselves, as these often do not match what other, nonaffected people assume.
Our findings indicate that optimal care should focus not only on physical health, but also on promoting social integration and emotional support.
Finally, it is important to note that in our study we only look at average outcomes in order to identify differences. This also means that the majority of pretermborn individuals have a good quality of life.
Self and parentreported quality of life from adolescence to adulthood
For further information on bullying, here is a link to a radio lecture by Professor Wolke, colead of the BLS: http://dradiowissen.de/beitrag/mobbing-auch-im-erwachsenenalter-nicht-vergessen
You know that we would like to stay in contact with you. Therefore, once again the request to inform us of any changes in address or telephone number. We continue to wish you all the best and a pleasant time.
Warm greetings from the BEST team at the study office in Bonn,
Prof.Dr. Dr. Peter Bartmann Dr. Barbara Busch